|
Overview
 A bunion, also known by its medical name hallux abductovalgus, is foot condition in which your big toe points toward your second toe, causing a bump or prominence to develop on the inside edge of your big toe and first metatarsal bone. Your first metatarsal bone is the long bone located directly behind your big toe, in your mid-foot. A bunion will cause your forefoot to appear wider because the base of your big toe now points away from your foot instead of pointing straight ahead. A bunion, also known by its medical name hallux abductovalgus, is foot condition in which your big toe points toward your second toe, causing a bump or prominence to develop on the inside edge of your big toe and first metatarsal bone. Your first metatarsal bone is the long bone located directly behind your big toe, in your mid-foot. A bunion will cause your forefoot to appear wider because the base of your big toe now points away from your foot instead of pointing straight ahead.Causes You may get bunions if the way your foot is shaped puts too much pressure on your big toe joint. Because bunions can run in families, some experts believe that the inherited shape of the foot makes some people more likely to get them. Your foot rolls inward too much when you walk. A moderate amount of inward roll, or pronation, is normal. But damage and injury can happen with too much pronation. You have flat feet. You often wear shoes that are too tight. All of these may put pressure on the big toe joint. Over time, the constant pressure forces the big toe out of alignment, bending it toward the other toes. Symptoms A bunion, also called a hallux valgus, is a bony prominence on the inside of the big toe, caused by a misalignment of the joint. The overlying skin maybe swollen, red and tender. Bunions are often painful and can limit what shoes you can wear. Diagnosis Diagnosis begins with a careful history and physical examination by your doctor. This will usually include a discussion about shoe wear and the importance of shoes in the development and treatment of the condition. X-rays will probably be suggested. This allows your doctor to measure several important angles made by the bones of the feet to help determine the appropriate treatment. Non Surgical Treatment Some bunions can be treated without surgery. If you have a bunion, wear shoes that are roomy enough so that they won?t put pressure on it. You can choose to have your shoes stretched out professionally or try cushioning the painful area with protective pads. Orthotics have been shown to help prevent progression of bunions. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Applying an ice pack several times a day can also help reduce inflammation and pain. If your bunion progresses to a point where you have difficulty walking or experience pain even with accommodative shoes, surgery may be necessary.  Surgical Treatment Severe cases may require, along with surgery, cast immobilization and prolonged avoidance of weight-bearing activity. You should know that undergoing surgery for this health problem does not guarantee a cure or even a beneficial health outcome. Bunions, like many other foot conditions, should always be approached from a prevention standpoint, or therapy should be directed at slowing the progression of your deformity. Overview
If you've been running long enough, you've most likely had to deal with various aches and pains in your feet, knees, hips or lower back. Plantar fasciitis, achilles tendinitis, IT-band syndrome, meniscus tears, runner's knee, bursitis of the hip or knee, patellofermoral pain syndrome, chondromalacia patella, lower back pain and piriformis syndrome are only some of many conditions an athlete may develop during the course of his or her running career.  Causes A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development. Symptoms People with overpronation may suffer from pain in the knees, hips, and low back. Overpronation itself does not necessarily cause any other symptoms but is a contributing factor of many foot conditions such as Plantar Facsiitis, Heel Spur Syndrome, Posterior Tibialis Tendon Rupture or Tendonitis, Hallux Valgus, Bunion Deformities, Metatarsalgia, Hallux Limitus or Hallux Rigidus, Hammer Toes, and Morton?s Neuroma. Diagnosis Look at your soles of your footwear: Your sneaker/shoes will display heavy wear marks on the outside portion of the heel and the inside portion above the arch up to the top of the big toe on the sole. The "wet-foot" test is another assessment. Dip the bottom of your foot in water and step on to a piece of paper (brown paper bag works well). Look at the shape of your foot. If you have a lot of trouble creating an arch, you likely overpronate. An evaluation from a professional could verify your foot type.  Non Surgical Treatment No matter what the cause in your case, over pronation can be remedied in several ways. Those who are overweight should consider permanently losing weight to naturally alleviate pressure on the ligaments and heel of the foot. Also, you should consult a podiatrist to examine your posture and movement habits. You may be reinjuring yourself due to poor alignment without even knowing it. If you also have lower back problems, this could be a sign of over pronation as a result of misalignment. Prevention Custom-made orthotics supports not only the arch as a whole, but also each individual bone and joint that forms the arch. It is not enough to use an over-the-counter arch support, as these generic devices will not provide the proper support to each specific structure of the arch and foot. Each pronated foot?s arch collapses differently and to different degrees. The only way to provide the support that you may need is with a custom-made device. This action of the custom-made orthotic will help to prevent heel spurs, plantar fasciitis, calluses, arch pain, and weakness of the entire foot. Overview
Sever?s Disease is often misdiagnosed as a simple growing pains and affects boys far more often than girls, especially between the ages of 8 and 14. It is extremely common in children that play Soccer, Basketball, And Hockey. However it is not limited to these sports alone, nor is it simply a pre-season type condition related to fitness. Sever?s Disease sounds terrible, but there is no need to panic as it is not a contagious or incurable condition. In children, there is a growth plate in the heel bone, which at puberty becomes solid and forms part of the heel, however prior to puberty it can cause pain if the child?s foot rolls inwards or outwards too much, causing increased stress on this growth plate and inturn causes pain. Causes Sever?s disease is often associated with a growth spurt, when the bones grow but the muscles do not. Therefore the muscles effectively become tighter which results in increased stress at the heel. It may also be related to unusual biomechanics, for instance poor foot posture, muscle tightness or muscle weakness. Overtraining or incorrect training can also play a part. Usually, the cause is a combination of factors. Symptoms The symptoms of Sever?s Disease may vary but usually include generalised pain and discomfort around the back of the heel. Can be one sided or both sides. Starts after child starts a new sport season. May cause child to limp due to pain. Increases with weight bearing activity. Heel becomes red and can be swollen. X-rays are usually inconclusive and simply show the growth plate. Diagnosis A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage. Non Surgical Treatment Depending on the underlying cause, treatment can include. Arch supports (foot orthoses) to correctly support the feet. Proper taping of the foot and heel. Rest from activities. Icing at the end of the day. A night splint worn at night. Flexibility exercises and strengthening. Ultrasound therapy. Anti-inflammatory drugs. Surgical Treatment The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon. Overview
The plantar fascia is a sturdy structure but the degree of stress that it takes makes it susceptible to injury. A force equal to almost three times body weight passes through the foot with each step. On running, this typically happens about 90 times a minute. Plantar fasciitis is thought to be a traction and overuse injury. Damage to the plantar fascia is usually in the form of micro-tears. It is a degenerative rather than an inflammatory process. Damage tends to occur near the heel, where stress on the fibres is greatest, and where the fascia is the thinnest. The fascia broadens as it extends toward the toes. Plantar fasciitis is often associated with calcaneal spurs. These are depositions of calcium where the fascia suffers most damage. Spurs are most commonly on the medial side at the origin of the fascia from the calcaneum. Spurs are the result of the process of plantar fasciitis and not the cause of the pain. It can present bilaterally.  Causes There are a variety of causes of flat feet. Flat feet can be genetic, acquired and develop over time. Young children and teens can have no arches. Injury can lead to flat feet. Tendon problems, and arthritis can lead to flat feet. Rigid flat feet may occur from a condition called tarsal coalition, where the bones in the back of the foot are genetically fused or locked together. Symptoms Go to a podiatrist at the first sign of symptoms. Besides pain on the bottom of the foot, additional symptoms may include. Burning sensation in arch. Difficulty standing on tiptoes. Inflammation. More pain after sleeping or resting. Redness. Heat. Localized pain in the ball of the foot. Sharp or shooting pain in the toes. Pain that increases when toes are flexed. Tingling or numbness in the toes. Aching. Pain that increases when walking barefoot. Pain that increases when walking on hard surfaces. Pain the increases when standing (putting weight on your feet) or moving around and decreases when immobile. Skin Lesions. It?s important to get a proper diagnosis and treatment plan. Let?s go over the possible causes of the pain. Diagnosis In more difficult cases of plantar fasciitis you should see your foot health professional for a thorough examination. They will find out why your arch or heel pain occurred in the first place and devise a treatment plan to relieve your pain and prevent it from reoccurring. They will evaluate your feet, walking pattern (gait), shoes, activities, exercise methods, and other relevant information and then devise your treatment plan. Non Surgical Treatment A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.  Surgical Treatment The main goal of surgery is to reduce pain and improve function. It may also reduce other injuries such as repeated ankle sprains and broken bones. Surgery may be considered if there is no relief with physical therapy, changes in shoewear and/or changes in activity. Some patients will also have tendon problems, ankle weakness and foot fractures. These patients may require other procedures to address related problems. If you have medical problems that make surgery unsafe, any infections or blood vessel disease, cavus foot surgery may not be appropriate. The surgical procedures involved with the correction of the cavus foot are varied. Theses may include correction of the bony deformity, ankle looseness and the muscle imbalances that cause the deformity. The goal is to provide a foot that evenly distributes weight along both inside and outside edges. A variety of incisions may be needed to perform the procedures related to the correction of the cavus foot. Stretching Exercises Plantar Fasciitis stretches should always be gentle and pain free, if discomfort occurs with or after stretching decrease the intensity and duration of stretches. Stretches can usually be gradually progressed in intensity and duration over time according to individual tolerance. Plantar Fasciitis Stretch 1. Stretch for the right calf muscle (gastrocnemius) and the arch of the right foot (plantar fascia and muscles under the arches). Take your right heel close to the wall and ball of the foot upright against the wall. Move your hips forwards to the wall. Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 2. Stretch for the outside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot outwards to 2 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the left). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 3. Stretch for the inside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot inwards to 10 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the right). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 4. Stretch for the right achilles tendon and the arch of the right foot. Take your right heel close to the wall and ball of the foot upright against the wall (as for stretch 1). Move your hips forwards to the wall. Bend your right knee forwards into the wall keeping the ball of your foot upright against the wall. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times.
Overview
Flatfoot deformity is a general term used to describe a person whose arches are slowly dropping to the ground, aka ?fallen arches.? Adult-acquired flatfoot deformity can be caused by several factors, but the most common is abnormal functioning of the posterior tibial tendon in the foot and ankle. The posterior tibial tendon is the primary tendon that supports the arch. If this tendon begins to elongate from a sustained, gradual stretch over a long period of time, then the arch will progressively decrease until full collapse of the arch is noted on standing. What makes this tendon elongated? Biomechanical instability of the foot such as over-pronation or an accessory bone at the insertion site of the tendon are the primary causes for posterior tibial tendon dysfunction.  Causes As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. Symptoms Most people will notice mild to extreme pain in their feet. Below outlines some signs and symptoms of AAFD. Trouble walking or standing for any duration. Pain and swelling on the inside of the ankle. Bump on the bottom of the foot. Ulcer or wound developing on the outer aspects of foot. Diagnosis Observation by a skilled foot clinician and a hands-on evaluation of the foot and ankle is the most accurate diagnostic technique. Your Dallas foot doctor may have you do a walking examination (the most reliable way to check for the deformity). During walking, the affected foot appears more pronated and deformed. Your podiatrist may do muscle testing to look for strength deficiencies. During a single foot raise test, the foot doctor will ask you to rise up on the tip of your toes while keeping your unaffected foot off the ground. If your posterior tendon has been attenuated or ruptured, you will be unable to lift your heel off the floor. In less severe cases, it is possible to rise onto your toes, but your heel will not invert normally. X-rays are not always helpful as a diagnostic tool for Adult Flatfoot because both feet will generally demonstrate a deformity. MRI (magnetic resonance imaging) may show tendon injury and inflammation, but can?t always be relied on for a complete diagnosis. In most cases, a MRI is not necessary to diagnose a posterior tibial tendon injury. An ultrasound may also be used to confirm the deformity, but is usually not required for an initial diagnosis. Non surgical Treatment A painless flatfoot that does not hinder your ability to walk or wear shoes requires no special treatment or orthotic device. Other treatment options depend on the cause and progression of the flatfoot. Conservative treatment options include making shoe modifications. Using orthotic devices such as arch supports and custom-made orthoses. Taking nonsteroidal anti-inflammatory drugs such as ibuprofen to relieve pain. Using a short-leg walking cast or wearing a brace. Injecting a corticosteroid into the joint to relieve pain. Rest and ice. Physical therapy. In some cases, surgery may be needed to correct the problem. Surgical procedures can help reduce pain and improve bone alignment. Surgical Treatment For more chronic flatfoot pain, surgical intervention may be the best option. Barring other serious medical ailments, surgery is a good alternative for patients with a serious problem. There are two surgical options depending on a person?s physical condition, age and lifestyle. The first type of surgery involves repair of the PTT by transferring of a nearby tendon to help re-establish an arch and straighten out the foot. After this surgery, patients wear a non-weight bearing support boot for four to six weeks. The other surgery involves fusing of two or three bones in the hind foot below the ankle. While providing significant pain relief, this option does take away some hind foot side-to-side motion. Following surgery, patients are in a cast for three months. Surgery is an effective treatment to address adult-acquired flatfoot, but it can sometimes be avoided if foot issues are resolved early. That is why it is so important to seek help right away if you are feeling ankle pain. But perhaps the best way to keep from becoming flatfooted is to avoid the risk factors altogether. This means keeping your blood pressure, weight and diabetes in check.
Overview
 The Achilles tendon is an important part of the leg. It is located just behind and above the heel. It joins the heel bone to the calf muscles. Its function is to help in bending the foot downwards at the ankle (this movement is called plantar flexion by doctors). If the Achilles tendon is torn, this is called an Achilles tendon rupture. The tear may be either partial or complete. In a partial tear, the tendon is partly torn but still joined to the calf muscle. With complete tears, the tendon is completely torn so that the connection between the calf muscles and the ankle bone is lost. Causes Your Achilles tendon helps you point your foot downward, rise on your toes and push off your foot as you walk. You rely on it virtually every time you move your foot. Rupture usually occurs in the section of the tendon located within 2.5 inches (6 centimeters) of the point where it attaches to the heel bone. This section may be predisposed to rupture because it gets less blood flow, which may impair its ability to heal. Ruptures often are caused by a sudden increase in the amount of stress on your Achilles tendon. Common examples include increasing the intensity of sports participation, falling from a height, stepping into a hole. Symptoms Patients present with acute posterior ankle/heel pain and may give a history of ?felt like someone kicked me from behind?. Patients may report a direct injury, or report the pain started with jumping or landing on a dorsiflexed foot. It is important to elicit in the history any recent steroid or flouroqunolone usage including local steroid injections, and also any history of endocrine disorders or systemic inflammatory conditions. Diagnosis A detailed history, and examination by an appropriately qualified health professional, will allow a diagnosis to be made. An ultrasound or MRI scan can confirm the diagnosis. Other causes of symptoms in the area, such as those referred from the lumbar spine and local infection, should be excluded. Non Surgical Treatment The best treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel; this allows the ends of your torn tendon to heal. This method can be effective, and it avoids the risks, such as infection, associated with surgery. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult. The Achilles tendon is an important part of the leg. It is located just behind and above the heel. It joins the heel bone to the calf muscles. Its function is to help in bending the foot downwards at the ankle (this movement is called plantar flexion by doctors). If the Achilles tendon is torn, this is called an Achilles tendon rupture. The tear may be either partial or complete. In a partial tear, the tendon is partly torn but still joined to the calf muscle. With complete tears, the tendon is completely torn so that the connection between the calf muscles and the ankle bone is lost. Causes Your Achilles tendon helps you point your foot downward, rise on your toes and push off your foot as you walk. You rely on it virtually every time you move your foot. Rupture usually occurs in the section of the tendon located within 2.5 inches (6 centimeters) of the point where it attaches to the heel bone. This section may be predisposed to rupture because it gets less blood flow, which may impair its ability to heal. Ruptures often are caused by a sudden increase in the amount of stress on your Achilles tendon. Common examples include increasing the intensity of sports participation, falling from a height, stepping into a hole. Symptoms Patients present with acute posterior ankle/heel pain and may give a history of ?felt like someone kicked me from behind?. Patients may report a direct injury, or report the pain started with jumping or landing on a dorsiflexed foot. It is important to elicit in the history any recent steroid or flouroqunolone usage including local steroid injections, and also any history of endocrine disorders or systemic inflammatory conditions. Diagnosis A detailed history, and examination by an appropriately qualified health professional, will allow a diagnosis to be made. An ultrasound or MRI scan can confirm the diagnosis. Other causes of symptoms in the area, such as those referred from the lumbar spine and local infection, should be excluded. Non Surgical Treatment The best treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel; this allows the ends of your torn tendon to heal. This method can be effective, and it avoids the risks, such as infection, associated with surgery. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult.  Surgical Treatment Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks. Surgical Treatment Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks.
Overview
 The Achilles tendon is the tough sinew that attaches the calf muscle to the back of the calcaneus, or heel bone. It is also known as the tendo calcaneus or the tendo Achilles and happens to be one of the longest tendons in the body. An Achilles tendon rupture occurs when the Achilles tendon is partially or completely broken or torn. The average age of patients who suffer Achilles tendon ruptures is 30 to 40 years. The male-to-female ratio is nearly 20 to 1. The Achilles tendon is the tough sinew that attaches the calf muscle to the back of the calcaneus, or heel bone. It is also known as the tendo calcaneus or the tendo Achilles and happens to be one of the longest tendons in the body. An Achilles tendon rupture occurs when the Achilles tendon is partially or completely broken or torn. The average age of patients who suffer Achilles tendon ruptures is 30 to 40 years. The male-to-female ratio is nearly 20 to 1.Causes A rupture occurs when a patient overstretches the Achilles tendon, an act which causes it to tear partially or completely. Achilles tendon ruptures can occur during athletic play or any time the tendon is stretched in an unexpected way. Symptoms Patients often describe a feeling of being kicked or hit with a baseball bat in the back of the heel during athletic activity. They are unable to continue the activity and have an extreme loss of strength with the inability to effectively walk. On physical examination there is often a defect that can be felt in the tendon just above the heel. A diagnosis of an Achilles tendon rupture is commonly made on physical exam. An MRI may be ordered to confirm the suspicion of a tear or to determine the extent of the tear. Diagnosis It is usually possible to detect a complete rupture of the Achilles tendon on the history and examination. A gap may be felt in the tendon, usually 4-5cm above the heel bone. This is the normal site of injury and is called an intra-substance tear. The tear can occur higher up about 10cm above the insertion into the heel at the site where the muscles join the tendon, this is known as a musculo-tendinous tear. A special test will be performed which involves squeezing the calf. Normally if the Achilles tendon is intact this causes the foot to point downwards but if it is ruptured it causes no movement. To confirm the diagnosis and the exact site of the rupture it may be necessary to perform an Ultra-sound or MRI scan. Non Surgical Treatment This condition should be diagnosed and treated as soon as possible, because prompt treatment probably improves recovery. You may need to be referred urgently to see a doctor in an orthopaedic department or accident and emergency department. Meanwhile, if a ruptured Achilles tendon is suspected, you should not put any weight on that foot, so do not walk on it at all.Treatment options for an Achilles tendon rupture include surgical and non-surgical approaches. The decision of whether to proceed with surgery or non-surgical treatment is based on the severity of the rupture and the patients health status and activity level. Non-surgical treatment, which is generally associated with a higher rate of re-rupture, is selected for minor ruptures, less active patients, and those with medical conditions that prevent them from undergoing surgery. Non-surgical treatment involves use of a cast, walking boot, or brace to restrict motion and allow the torn tendon to heal. 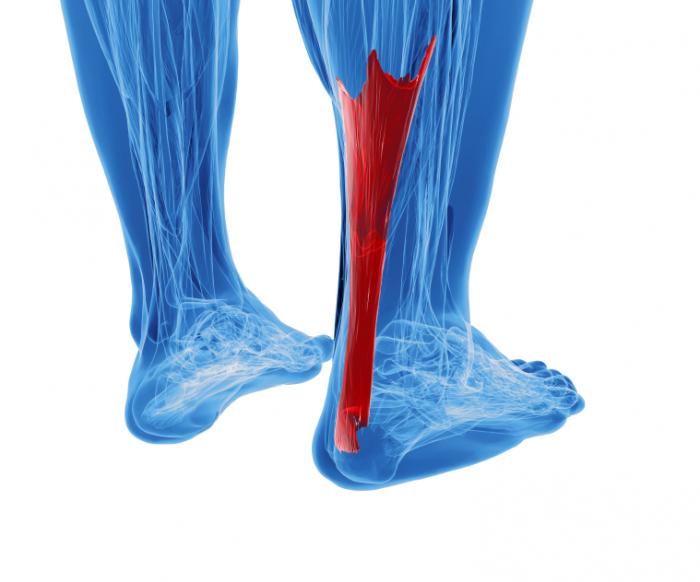 Surgical Treatment There are a variety of ways to repair an Achilles tendon rupture. The most common method is an open repair. This starts with an incision made on the back of the lower leg starting just above the heel bone. After the surgeon finds the two ends of the ruptured tendon, these ends are sewn together with sutures. The incision is then closed. Another repair method makes a small incision on the back of the lower leg at the site of the rupture. A series of needles with sutures attached is passed through the skin and Achilles tendon and then brought out through the small incision. The sutures are then tied together. The best surgical technique for your Achilles rupture will be determined by your orthopaedic foot and ankle surgeon. |
